
The Honest Problem
Road to CEPAS 2026 — Episode 1

In late October 2026 I’ll stand on a stage in Lyon for twenty minutes and talk about big data, AI, and sepsis prediction in the NICU. The session is called Omics in Sepsis. The venue is the first Congress of the European Paediatric Academic Societies. I said yes the moment the invitation arrived.
I’ve been quietly uneasy about it ever since.
Not about the speaking part, that’s familiar territory. The unease is about what I’m supposed to say. Because if I’m honest with the audience, and I intend to be, the talk has to begin with a problem most of us in this field have stopped acknowledging out loud.
ChatGPT Image 2
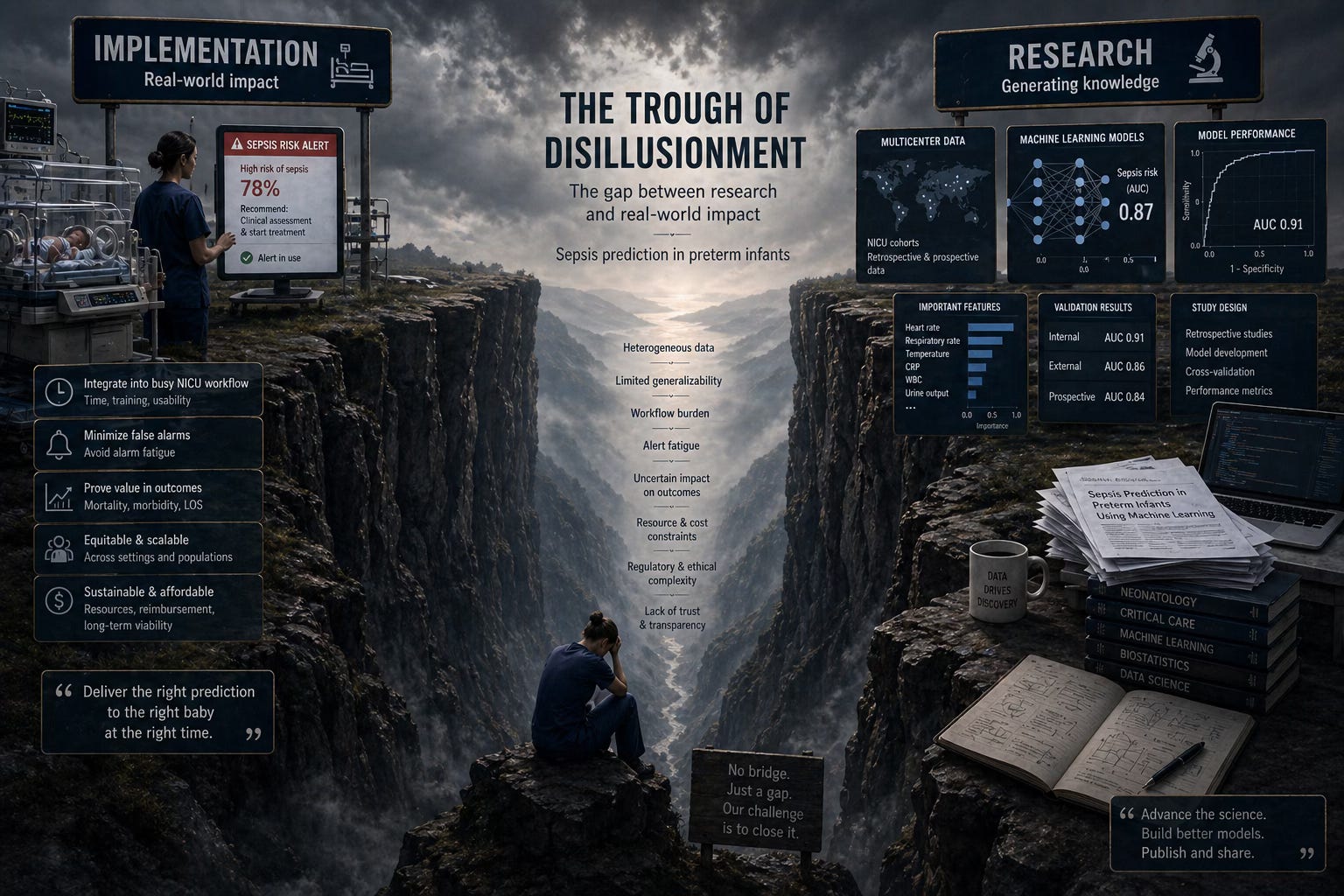
We can predict. So what?
We can predict late-onset sepsis in preterm neonates reasonably well, and we have been able to for years. The literature is full of models. ROC curves climbing toward 0.80, 0.85, occasionally higher with enough feature engineering and a cooperative dataset. That includes — full disclosure — our own paper from 2023 in Computers in Biology and Medicine. AUC 0.73 at the moment of clinical suspicion. A longitudinal impact simulation suggesting we could have flagged 47% of LOS cases ahead of the bedside team, while keeping false alarms below three per day. A genuinely useful exercise in clinical impact assessment, more than most papers in the space at the time.
It’s a good paper. I’m proud of the work. It is also a model that, as I write this in the spring of 2026, is not being used to take care of a single baby. Not in our NICU. Not anywhere.
That is the honest problem. Not can AI predict neonatal sepsis or at least clinical deterioration, that question is largely settled. The honest problem is the next one. Once we have the prediction, what do we actually do with it?
The HeRO question
Consider the HeRO monitor — heart rate characteristics, FDA-cleared, with a randomized trial showing absolute mortality reduction in very low birthweight infants. That trial was published in 2011. Fifteen years on, HeRO is on the market, the evidence is real, and yet ask any group of neonatologists how they respond when the score climbs and you’ll get a different answer at every cot. Order an IL-6? A CRP? Both? Neither? Increase observation? Start empiric antibiotics? Wait? Blood culture?
This is not a HeRO problem. It is the problem of every prediction tool we have built, including ours. We have invested decades into the predict half of the equation and almost nothing into the act half. There is no validated response protocol. No agreed-upon downstream pathway. No randomized comparison of “alarm fires → action A” versus “alarm fires → action B.” The score lights up and the clinical reasoning that follows is, essentially, vibes.
That is the gap I want to talk about in Lyon. Not the success stories. The gap.
What this project is
So, between now and 31 October 2026, I’m going to build the talk in public. Twenty-some weeks. Posts on this Substack, a growing public literature base, an AI-assisted mini systematic review along the way, and the slides themselves at the end. Everything sourced. Everything visible. Nothing dressed up.
I’m doing it with Claude as a research partner. Not as a gimmick, as the actual working method. PubMed searches, evidence tables, critical re-reads of papers (including my own), regulatory landscape mapping, slide logic. Every post will include a short “How I used Claude” section so you can see exactly where the AI helped and where it didn’t. If you want to copy the workflow for your own project, you’ll have everything you need.
The thesis I’ll keep returning to is simple. Prediction is not clinical utility, and the field has not yet built the bridge between them. That bridge is regulatory, methodological, behavioural, and economic. Each of the next posts is a piece of it.
How I used Claude in this post
I drafted the framing and the argument. Claude turned the bullet points of the project brief, the CEPAS invitation, the paper details, the “dal” I find myself in, into structured prose, kept the word count in range, and pushed back on a softer opening I’d originally written. I edited every paragraph. The unease is mine.
What’s next
Episode 2 lands soon: Searching the Evidence — Live. I’ll run a real PubMed search for LOS prediction models with Claude using the PubMed MCP, on screen, queries and all. If you want to follow along or copy the method, subscribe, and meet me in Lyon, virtually or otherwise.
More will appear soon @ neonatology.ai.
NB the images will become more happy along the way